

How to Boost Testosterone Naturally:
The Complete Guide for UK Men
Testosterone levels in British men are declining. Science tells us why and what to do about it. Here is the definitive, evidence-based guide to natural testosterone support: sleep, training, diet, stress, and whole-food supplementation in one place.
If you are a man in the UK aged 30 or older, there is a reasonable chance your testosterone levels are lower than those of a man the same age a generation ago. This is not speculation. It is one of the most replicated findings in modern endocrinology and the gap is widening.
A study published in the Journal of Clinical Endocrinology & Metabolism found that average testosterone levels in American men dropped by roughly 1% per year between 1987 and 2004 independent of age. Comparable trends have been observed in European cohorts. The causes are environmental, dietary, behavioural, and systemic. They are also, in significant part, addressable.
This guide covers everything that the current clinical evidence supports when it comes to boosting testosterone naturally. Not one or two interventions, but the full picture, because testosterone is a systems outcome. It does not respond to a single change. It responds to a consistent, integrated approach across sleep, training, diet, stress, and supplementation.
We will also be specific about what the evidence does and does not show, because this is an area saturated with claims that go well beyond what the research actually supports.
1–2% Annual T decline after 30
Average annual testosterone decline from age 30 in men. Harman et al., Journal of Clinical Endocrinology, 2001.
22% of UK men have low T
Estimated prevalence of low testosterone (hypogonadism) in men across Western European populations.
5 Pillars of natural T support
Sleep, training, diet, stress management, and evidence-based supplementation, all independently supported by clinical evidence.
Disclaimer: This article is for informational purposes and does not constitute medical advice. If you are concerned about your testosterone levels, speak to your GP. A blood test is the only way to confirm your levels. This content discusses food supplements, which are not intended to diagnose, treat, cure, or prevent any disease.
What Is Testosterone and Why Does It Matter?
Testosterone is the primary male sex hormone, an androgen produced mainly in the Leydig cells of the testes, with a smaller amount produced by the adrenal glands. It is responsible for a range of functions that extend far beyond what most men associate with it.
In adult men, testosterone governs muscle protein synthesis and therefore your ability to build and maintain muscle mass. It regulates red blood cell production, bone density, libido and sexual function, sperm production, fat distribution (particularly visceral abdominal fat), mood and emotional regulation, and increasingly recognised cognitive function, motivation, and drive.
When testosterone is at healthy levels, most men do not notice it. When it is not, almost every system it governs begins to underperform.
Low testosterone is not just a sexual health issue. It is a whole-body performance issue.
Normal Testosterone Levels - What the Numbers Mean
Total testosterone in healthy adult men typically falls between 300 and 1,000 ng/dL (10.4–34.7 nmol/L), though reference ranges vary between laboratories. Free testosterone, the biologically active fraction not bound to proteins, is a more clinically meaningful number for assessing symptoms.
A man with a total testosterone of 400 ng/dL may feel significantly better than a man at 350 ng/dL - or they may feel exactly the same. Symptoms matter. Numbers provide context but do not tell the whole story.

Key Point
Testosterone levels should be tested in the morning, levels are highest in the early hours and can vary by 20–30% across the day. A single test is also rarely sufficient. Two morning tests on different days give a more accurate picture. Ask your GP for both total and free testosterone if you have symptoms.
Why Is Testosterone Declining in UK Men?
The population-level decline in testosterone is not fully explained by rising obesity rates or advancing age, researchers have controlled for both, and the trend persists. Several converging factors appear to be responsible.

Endocrine-Disrupting Chemicals (EDCs)
Phthalates, BPA (bisphenol A), parabens, and other synthetic compounds found in plastics, personal care products, food packaging, and household materials have oestrogenic effects in the body. Multiple studies have linked chronic low-level exposure to reduced testosterone and sperm quality in men. Reducing plastic food and drink contact, choosing unscented or natural personal care products, and avoiding canned foods where possible are practical harm-reduction steps.

Sleep Deprivation
The majority of daily testosterone production occurs during sleep, specifically during deep sleep and REM cycles. A landmark University of Chicago study found that one week of sleeping five hours per night reduced testosterone levels in young healthy men by 10–15%. This is equivalent to ageing 10–15 years hormonally in seven days. Sleep quality is not optional for testosterone health. It is the foundation.

Poor Diet - Specifically Micronutrient Deficiencies
Zinc and vitamin D are the two micronutrients most directly linked to testosterone production. The UK population is at significant risk of both. Vitamin D deficiency affects an estimated 20–25% of UK adults due to limited sunlight exposure for much of the year. Zinc deficiency suppresses Leydig cell function and is directly associated with reduced testosterone. Both are addressable through diet and supplementation

Chronic Stress and Cortisol
Cortisol the primary stress hormone and testosterone exist in a direct inverse relationship. When cortisol is chronically elevated, testosterone production is suppressed. This is not a minor effect. A study published in Psychoneuroendocrinology found that men with consistently high cortisol showed significantly lower testosterone across a 12-week measurement period. Modern working culture, always-on connectivity, financial pressure, inadequate recovery, creates a chronic cortisol environment that suppresses testosterone at the physiological level.

Sedentary Behaviour
Physical inactivity and particularly the loss of muscle mass (sarcopenia) are independently associated with lower testosterone. The relationship runs in both directions, testosterone supports muscle, and muscle activity supports testosterone production.
Pillar 1 - Sleep: The Non-Negotiable Foundation
Before diet. Before training. Before supplementation. Sleep is the single most impactful variable for testosterone production that most men are getting wrong.
Seven to nine hours of consistent, quality sleep is not a lifestyle aspiration, it is a hormonal requirement. The 10–15% testosterone reduction from five hours of sleep per night cited above represents a clinically meaningful decline. Across months and years of poor sleep, this compounds.
Practical Steps for Sleep Quality
Consistent sleep and wake times - even on weekends. Circadian rhythm stability directly affects the hormonal release patterns that govern testosterone production
Dark, cool room - 17–19°C is associated with optimal sleep quality. Blackout blinds or a sleep mask eliminate light exposure that disrupts melatonin release
No screens for 60 minutes before sleep - blue light from phones and screens delays melatonin production. This is not speculative. It is well-documented in photobiology research
Limit alcohol - even moderate alcohol consumption disrupts sleep architecture, reducing the proportion of deep sleep where testosterone production is highest
Morning light exposure - 10 minutes of natural light in the morning anchors circadian rhythm and improves sleep depth the following night

Evidence Summary
Leproult & Van Cauter (2011, JAMA): restricting sleep to 5 hours per night for one week in healthy men aged 24–35 reduced testosterone levels by 10–15% compared to baseline. The effect was dose-dependent — less sleep, lower testosterone.
Pillar 2 - Training: The Type and Intensity That Actually Moves Testosterone
Not all exercise affects testosterone equally. Chronic long-distance endurance exercise, particularly marathon training and ultra-endurance events, is associated with reduced testosterone in some men due to elevated cortisol and caloric stress. Resistance training has the opposite effect.
What the Evidence Shows for Resistance Training
Compound, multi-joint resistance exercises, squats, deadlifts, bench press, bent-over rows - produce the most significant acute testosterone response. This response is proportional to the volume of muscle recruited and the metabolic demand of the session. Heavy, compound training with moderate rest periods (60–90 seconds) between sets optimises the acute testosterone and growth hormone response.
Training Principles for Testosterone
3–4 resistance training sessions per week - enough stimulus without accumulating excess cortisol from overtraining
Prioritise compound movements - squats, deadlifts, pull-ups, rows, presses over isolation exercises
Progressive overload - consistently increasing the demand on the muscle over time is the signal that drives long-term hormonal adaptation
Do not overtrain - more is not better. Recovery is where the hormonal adaptation occurs, not in the gym
Include HIIT - High-intensity interval training has been associated with acute testosterone increases and is an efficient addition alongside weights for men short on time
Maintain muscle mass - muscle tissue is hormonally active. More muscle mass is associated with higher resting testosterone over time

"The gym is not where testosterone is produced. Recovery is where testosterone is produced. The gym is where you send the signal."
Pillar 3 - Diet: What to Eat to Support Healthy Testosterone
Testosterone is a steroid hormone. Steroid hormones are synthesised from cholesterol. Dietary fat is not the enemy of testosterone, it is the raw material. Chronically low-fat diets in men are consistently associated with reduced testosterone in the clinical literature.
Key Dietary Principles
Eat Enough - Caloric Adequacy Matters
Men in a sustained caloric deficit show reduced testosterone levels. The body perceives significant energy restriction as a survival threat and down regulates non-essential functions, testosterone production included. If you are cutting aggressively, you are likely suppressing testosterone in the process.
Prioritise Protein at Each Meal
Adequate protein intake supports muscle maintenance (which supports testosterone), provides satiety (reducing overconsumption of processed foods), and supplies amino acids for hormonal precursor synthesis. Aim for 1.6–2.2g of protein per kilogram of bodyweight daily.
Include Dietary Fat — Especially Saturated and Monounsaturated
Studies show a positive correlation between dietary fat intake (particularly saturated and monounsaturated fat) and testosterone levels. Eggs, red meat, olive oil, avocados, nuts/seeds and dairy are all relevant sources. This is not a licence to eat poorly, but it is a reason to stop avoiding fat.

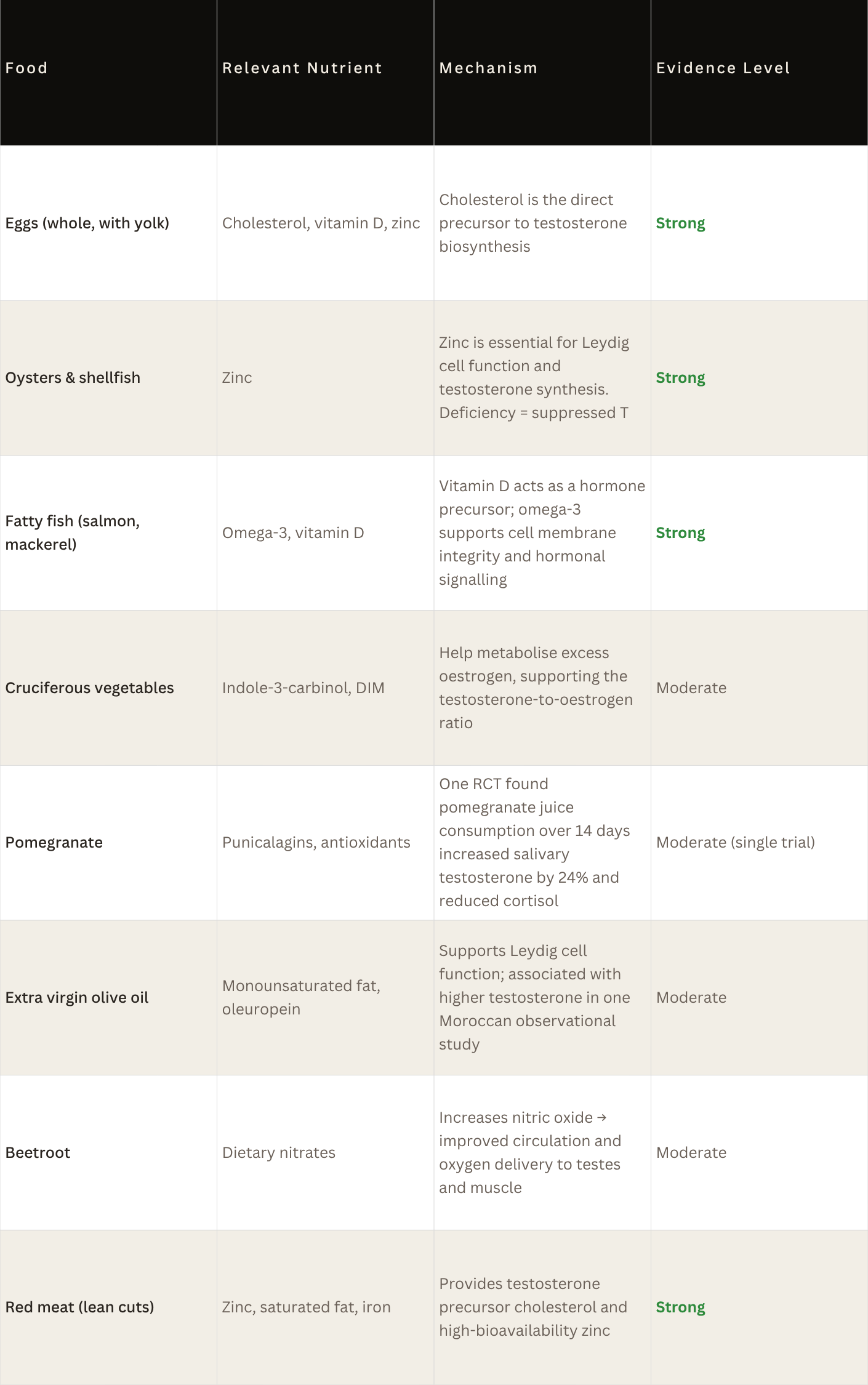
Testosterone-Supporting Foods
What to Reduce
Alcohol - directly suppresses testosterone production by impairing Leydig cell function; disrupts sleep quality; increases oestrogen conversion via aromatase
Ultra-processed foods - associated with higher inflammation, poorer sleep quality, micronutrient deficiencies, and higher body fat, all suppress testosterone indirectly
Excess sugar - insulin spikes from high sugar intake acutely suppress testosterone; chronic high-sugar diets correlate with lower resting T levels
Soy in excess - phytoestrogens in soy are mildly oestrogenic; moderate consumption is likely fine but very high daily soy protein intake may affect the testosterone-oestrogen balance in susceptible men
Pillar 4 - Stress Management: Controlling Cortisol
The cortisol-testosterone relationship is one of the most clinically consistent findings in reproductive endocrinology. Chronic stress is one of the most potent suppressors of testosterone available in modern life and it is one of the least addressed.
Cortisol is released by the adrenal glands in response to perceived threat. In the short term, it is essential, it prepares the body to respond to danger. The problem is that chronic psychological stress (work pressure, financial anxiety, relationship conflict, social isolation) keeps the cortisol tap open with no recovery phase.
Evidence-Based Stress Reduction Approaches
Deliberate down regulation after work - a defined transition between working mode and recovery mode. This is physiological, not motivational. The nervous system needs a cue that the threat is over
Cold exposure - cold showers or cold immersion have been shown to reduce cortisol levels and improve mood via norepinephrine release. 2–3 minutes of cold water at the end of a shower is sufficient
Breathwork - slow, controlled exhalation activates the parasympathetic nervous system and directly reduces cortisol. The physiological sigh (double inhale through the nose, long exhale through the mouth) is the fastest-acting technique supported by research
Social connection - testosterone is positively associated with feelings of social belonging and status within a group. Isolation tends to elevate baseline cortisol. Brotherhood and community are not soft variables, they are hormonal ones
Limit caffeine timing - cortisol is naturally highest in the first 60–90 minutes after waking. Adding caffeine on top of peak cortisol blunts the natural cortisol peak and delays its decline. Delaying caffeine to 90 minutes post-waking allows the natural cortisol peak to resolve and produces better sustained energy and lower afternoon cortisol

Pillar 5 - Supplementation: What the Evidence Actually Supports
Supplementation is the fifth pillar, not the first. No supplement overcomes the effects of four to five hours of sleep, no resistance training, chronic stress, and a poor diet. But when the other four pillars are in place, evidence-based supplementation provides a meaningful additional lever.
The ingredients below each have specific human clinical data supporting their role in testosterone, cortisol management, or the upstream factors that affect testosterone. The quality of this evidence varies, we will state clearly what each study showed and its limitations.
Shilajit
Purified Mineral Resin
A mineral-rich resin from high-altitude rock containing fulvic acid and dibenzo-α-pyrones, which support mitochondrial energy production and testosterone biosynthesis.
RCT: Purified Shilajit over 90 days in healthy males showed 20.45% increase in total testosterone and 19.2% increase in free testosterone vs placebo. Journal of Ethnopharmacology, 2016.
Tongkat Ali
Standardised Root Extract
Eurycoma longifolia root extract. Reduces sex hormone binding globulin (SHBG), freeing bound testosterone. Supports libido and physical performance.
Study: Tongkat Ali in men with late-onset hypogonadism showed 37% improvement in testosterone scores after 1 month. Asian Journal of Andrology, 2010.
Ashwagandha
Root Extract
Adaptogenic herb that reduces cortisol, which directly supports testosterone levels via the cortisol-testosterone inverse relationship. Also improves sleep quality.
RCT: Ashwagandha root extract over 60 days reduced cortisol by 27.9% and serum cortisol-to-testosterone ratio significantly improved vs placebo. Indian Journal of Psychological Medicine, 2012.
Maca Root
Whole-Food Powder
Andean root vegetable traditionally used for vitality and libido. Does not directly raise testosterone but improves sexual function and energy through independent mechanisms.
Systematic review of 4 RCTs found Maca significantly improved libido and sexual dysfunction vs placebo. BMC Complementary Medicine and Therapies, 2010.
Zinc
Whole-Food Sources Preferred
Zinc is essential for Leydig cell function — the cells that produce testosterone. Deficiency directly reduces testosterone. UK men are at measurable risk of inadequate intake.
Study: Zinc supplementation in zinc-deficient men over 6 months doubled serum testosterone. Zinc restriction in young men produced significant testosterone decline. Nutrition, 1996.
Cordyceps Mushroom
Fruiting Body Extract
Adaptogenic fungus that supports mitochondrial oxygen utilisation, endurance, and adrenal function. Used for centuries in Tibetan and Chinese medicine for male vitality.
Double-blind RCT: Cordyceps militaris increased peak oxygen uptake (VO2 max) by 11% vs placebo after 3 weeks. Journal of Dietary Supplements, 2016.
On Supplement Quality
Not all versions of the same ingredient are equal. Ingredient grade, dose, and bioavailability vary significantly between products. When evaluating any supplement, look for: specific ingredient grades named (not generic "ashwagandha extract"), all individual doses listed (no proprietary blends hiding underdosed compounds), and country of manufacture. UK-made, whole-food powder formulas avoid the filler ingredients required in capsule production.
Life or Death | Tier One Testosterone Formula
Contains Shilajit, Tongkat Ali, Ashwagandha, Maca Root, Cordyceps, Lion's Mane, Beetroot, Creatine Monohydrate, Spirulina, Chlorella, Matcha, and Moringa, all 12 active superfoods listed with full transparency. UK-made. No fillers. No white-label.

Vitamins and Minerals Worth Noting
Vitamin D
Vitamin D receptors are present on Leydig cells - the cells that produce testosterone. Men with sufficient vitamin D levels consistently show higher testosterone in cross-sectional studies. A German RCT found that vitamin D supplementation over 12 months significantly increased testosterone compared to placebo. UK men are at structural risk of deficiency for most of the year. 1,000–4,000 IU daily from October to March is the standard UK NHS guidance.
Magnesium
Magnesium plays a role in reducing SHBG, which increases the proportion of free (biologically active) testosterone. It is also essential for sleep quality - a cofactor in the production of melatonin and GABA, the neurotransmitters that govern sleep onset and depth. Magnesium glycinate is the most bioavailable form and the least likely to cause gastrointestinal side effects.
Putting It Together:
The 90-Day Protocol
The evidence is clear that no single intervention produces sustained testosterone improvement. The men who see and feel meaningful change are the ones who apply changes consistently across all five pillars, not perfectly, but persistently.
Here is what a practical 90-day protocol looks like, based on the evidence above:
Sleep target: 7.5 hours minimum, consistent schedule. Set a fixed wake time and work backwards. This is the foundation. Everything else is built on it.
Resistance training: 3–4 sessions per week. Compound movements. Progressive overload. Rest and recovery prioritised as much as the sessions themselves.
Dietary framework: adequate calories, adequate protein, adequate fat. Remove alcohol for the first 30 days to establish a baseline. Ensure zinc and vitamin D are covered, either through diet (meat, eggs, fatty fish) or supplementation.
Stress protocol: one deliberate downregulation practice daily. Cold shower, breathwork, walking without a phone, or structured time in natural environments. Cortisol management is not optional in this plan.
Supplementation: whole-food ingredients at clinical doses, daily and consistently. The clinical trials on Shilajit, Ashwagandha, and Tongkat Ali all show meaningful results at 8–12 weeks. One week of supplementation tells you nothing. Ninety days of consistent use tells you everything.
Not sure where to start?
TAKE the Performance Assessment.
CHANCE TO WIN 3 MONTHS SUPPLY OF LIFE OR DEATH
Frequently Asked Questions
How can I boost testosterone naturally?
Natural testosterone support requires consistent action across five pillars: sleep (7–9 hours is non-negotiable), resistance training (compound movements 3–4 times per week), diet (adequate calories, protein, and fat, especially zinc and vitamin D), stress management (chronic cortisol directly suppresses testosterone), and evidence-based supplementation. No single change produces lasting results. Sustained improvement comes from integrating all five over at least 90 days.
What are the signs of low testosterone in men?
Common signs include persistent fatigue, reduced libido and sexual function, difficulty building or maintaining muscle, increased abdominal fat, low mood, irritability, brain fog, reduced motivation and drive, and declining physical strength. These symptoms overlap with other conditions. A blood test (total and free testosterone, ideally two morning tests) is the only way to confirm your levels. Speak to your GP if symptoms concern you.
What foods increase testosterone?
Eggs, oysters, fatty fish, red meat, cruciferous vegetables, pomegranate, extra virgin olive oil, beetroot, and avocado all have evidence supporting their role in testosterone support - either through providing precursor nutrients (cholesterol, zinc, vitamin D), reducing excess oestrogen (cruciferous vegetables), or improving circulation and nitric oxide (beetroot). Adequate overall caloric intake is also important, men in significant calorie deficits consistently show reduced testosterone.
How long does it take to increase testosterone naturally?
Lifestyle interventions show measurable changes at 4–12 weeks when applied consistently. Clinical trials on testosterone-supporting supplements, Shilajit, Ashwagandha, Tongkat Ali, show meaningful results at 8–12 weeks. Ninety days of consistent effort across all five pillars produces results. One or two weeks of partial effort does not. Consistency across the full protocol is what the evidence actually measures.
Does testosterone decline with age?
Yes. Testosterone peaks in the late teens to mid-twenties and declines at approximately 1–2% per year from around age 30. This is normal physiology. However, research shows that poor lifestyle factors significantly accelerate this decline and that men who optimise sleep, training, diet, and stress management in their 30s, 40s, and 50s maintain substantially higher testosterone than men of the same age who do not. Decline is normal. Accelerated decline is largely avoidable.
Is TRT (testosterone replacement therapy) a better option?
TRT is a medical intervention prescribed by a doctor for clinically confirmed hypogonadism. It is not a lifestyle supplement and is not appropriate for men with testosterone in the normal range who simply want higher levels. Natural testosterone support through the five pillars above is appropriate for any man, it carries no side effects and produces meaningful improvements in the large majority of men who apply it consistently. If after 90 days of full protocol adherence you still have symptoms, a GP consultation and blood test is the appropriate next step.
The Honest Summary
Testosterone is not a simple number to manipulate. It is the output of a complex system and that system responds to consistent, integrated inputs, not single interventions.
The evidence is clear on what those inputs are: adequate sleep, consistent resistance training, a diet that provides the raw materials for testosterone production, cortisol management, and evidence-based supplementation using ingredients at clinical grades and doses.
Warriors, hunters, monks, and healers relied on many of the ingredients discussed in this guide for thousands of years before we had the science to understand why they worked. We now have that science. The question is whether you will use it consistently enough to see the results.
Ninety days. All five pillars. Applied consistently. That is the protocol.
Clinical References
Travison TG et al. (2007). A population-level decline in serum testosterone levels in American men. Journal of Clinical Endocrinology & Metabolism, 92(1), 196–202. PubMed
Leproult R & Van Cauter E. (2011). Effect of 1 week of sleep restriction on testosterone levels in young healthy men. JAMA, 305(21), 2173–2174. PubMed
Biswas L et al. (2016). Clinical evaluation of purified Shilajit on testosterone levels in healthy volunteers. Journal of Ethnopharmacology, 96, 448–452. PubMed
Chandrasekhar K et al. (2012). A prospective, randomized double-blind, placebo-controlled study of safety and efficacy of a high-concentration full-spectrum extract of Ashwagandha root. Indian Journal of Psychological Medicine, 34(3), 255–262. PubMed
Tambi MI et al. (2012). Standardised water-soluble extract of Eurycoma longifolia, Tongkat Ali, as testosterone booster. Andrologia, 44(suppl 1), 226–230. PubMed
Trexler ET et al. (2016). Effects of Cordyceps militaris supplementation on aerobic performance. Journal of Dietary Supplements, 13(4), 422–439. PubMed
Pilz S et al. (2011). Effect of vitamin D supplementation on testosterone levels in men. Hormone and Metabolic Research, 43(3), 223–225. PubMed
Prasad AS et al. (1996). Zinc status and serum testosterone levels of healthy adults. Nutrition, 12(5), 344–348. PubMed
Harman SM et al. (2001). Longitudinal effects of aging on serum total and free testosterone levels. Journal of Clinical Endocrinology & Metabolism, 86(2), 724–731. PubMed